
If you feel like HRT is not working, you are not alone. Many women find that their symptoms do not improve, or even worsen, when starting HRT for the first time.
Hormone replacement therapy (HRT) can be life changing for many women. For those struggling with symptoms of perimenopause and menopause such as poor sleep, anxiety, hot flushes, brain fog or low mood, replacing declining hormones can restore quality of life.
However, while HRT can be extremely beneficial, it is not always straightforward. Hormones interact with many systems in the body including the brain, liver, gut and stress response.
This means that the same HRT regime will not suit every woman and sometimes symptoms persist or even worsen if important factors are overlooked. Understanding the common pitfalls of HRT can help women make informed decisions and work with their clinician to create a treatment plan that truly supports their health.
Below are some of the most common issues that can arise when women start HRT and what can be done to address them.
1. Using synthetic progestins instead of progesterone
One of the most common misunderstandings around HRT relates to progesterone.
Women who take oestrogen therapy must also take a progesterone or progestogen to protect the lining of the womb from excessive thickening. However, not all forms of progesterone behave the same way in the body.
Many older HRT preparations contain synthetic progestins, which are chemically modified molecules designed to mimic some of the actions of progesterone. These compounds primarily act locally in the uterus to protect the endometrium.
By contrast micronised progesterone, which is bio identical progesterone chemically identical to the hormone produced in the body, has broader effects throughout the body including the brain.
Research shows that progesterone can be converted in the brain into neuroactive metabolites such as allopregnanolone, which act on GABA receptors and have calming and sleep promoting effects. This is one reason why oral micronised progesterone is often associated with improved sleep quality and reduced anxiety in menopausal women.
Synthetic progestins do not produce these neuroactive metabolites and in some cases may even produce unwanted side effects such as low mood, acne or breast tenderness.
The choice of progestogen therefore matters. This is often a key reason it may feel like your HRT is not working. While synthetic progestins are still widely used and may be appropriate for some women, at FUTURE WOMAN we favour micronised progesterone because it provides additional benefits for sleep, mood and cognitive symptoms.
2. Starting oestrogen too early or at too high a dose
Another common reason HRT is not working, is the assumption that perimenopausal symptoms are always due to low oestrogen. In reality the hormonal picture during perimenopause is much more complex. Research shows that progesterone levels decline earlier in the menopausal transition, largely because ovulation becomes less consistent. Oestrogen production, however, often remains relatively high and fluctuates widely during this time.
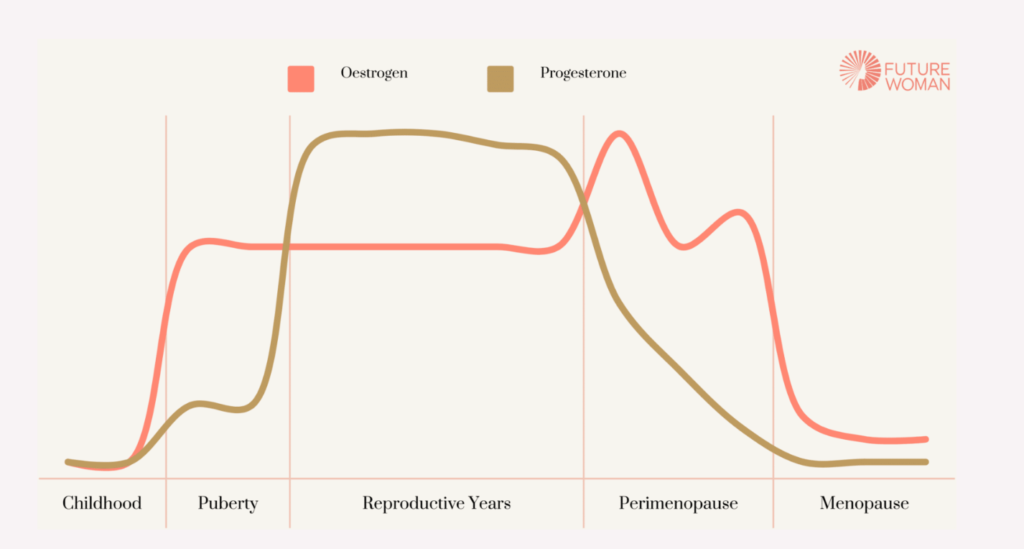
Studies of hormonal patterns across the menopausal transition show that oestradiol levels can sometimes be higher than those seen in reproductive years before eventually declining later in menopause. This means that in the early stages of perimenopause some women may actually experience symptoms of relative oestrogen excess, particularly if progesterone levels are falling.
Symptoms associated with oestrogen dominance may include heavy or prolonged bleeding,
breast tenderness, premenstrual mood changes, bloating and poor sleep.
If additional oestrogen, or combined HRT with a synthetic progestin, is introduced at this stage without assessing oestrogen:progesterone balance, symptoms may worsen rather than improve.
This does not mean oestrogen therapy should be avoided in early perimenopause. However it highlights the importance of testing first with a comprehensive test like the FUTURE WOMAN Advanced Hormone Test and making sure dosing is individualised and carefully monitored. This is particularly in women whose main complaints involve heavy periods or premenstrual type symptoms.
3. Not optimising estrogen metabolism
Hormone levels are only part of the story. How the body metabolises and clears hormones is equally important. Poor metabolism is often a key factor if HRT is not working.
Oestrogen is processed primarily in the liver through several metabolic pathways. The three main pathways produce metabolites known as 2 hydroxyoestrogen (2-OH), 4 hydroxyoestrogen (4-OH) and 16 hydroxyoestrogen (16-OH).
- The 2-OH pathway is generally considered the more favourable route and produces weaker oestrogenic compounds.
- The 16-OH pathway produces metabolites that bind more strongly to oestrogen receptors and may promote greater tissue stimulation. A predominance of this pathway has been associated with symptoms linked to higher oestrogen activity including breast tenderness and heavy bleeding.
- The 4-OH pathway can generate metabolites that are capable of forming reactive quinones which may contribute to oxidative DNA damage if not properly detoxified.
These metabolites normally undergo further detoxification through methylation, a biochemical process that requires nutrients such as folate, vitamin B12 and magnesium. If methylation processes are slow or inefficient, oestrogen metabolites may persist in circulation longer than intended. This can potentially contribute to symptoms of oestrogen excess even when hormone levels themselves appear normal.
For this reason it is important to consider supporting liver detoxification pathways and methylation status if experiencing persistent oestrogen dominant symptoms on HRT. The Advanced Hormone Test can check your estrogen metabolism and pathways along with how well you are methylating and detoxifying your estrogen.
Find out more about estrogen detoxification here.
4. Ignoring absorption and the role of gut health
HRT can be delivered through several routes including oral tablets, skin patches, gels or vaginal preparations. Each method has advantages and limitations. You may need to adjust if your HRT is not working.
Oral oestrogen is absorbed through the digestive system and then processed by the liver in what is known as first pass metabolism. This can influence the types of oestrogen metabolites produced and may also be affected by digestive health.
The gut microbiome plays a role in oestrogen metabolism through a group of bacterial enzymes known collectively as the estrobolome. Imbalances in gut bacteria may influence how oestrogen is reabsorbed or eliminated. Poor gut health or dysbiosis could therefore potentially influence how women respond to oral hormone therapy.
Transdermal preparations such as patches or gels bypass the digestive system and are absorbed through the skin. However this route can also be influenced by external factors including skin condition, sweating and the site of application.
Medications that can speed up liver metabolism can also affect HRT effectiveness and HRT may also be poorly absorbed when taken concurrently with GLP-1 medications such as Wegovy or Mounjaro, as these drugs function by slowing down stomach emptying. Conditions like IBS can also affect absorption of oral HRT because of a fast or slow transit time.
We believe it is therefore important to adjust the delivery method if symptoms do not improve with one form of therapy. Our bHRT clinic has a wide range of applications and doses which can be tailored to each individual based on symptoms and test results.
5. Assuming you are progesterone “intolerant“
Although progesterone is often calming for many women, some experience the opposite effect. This has sometimes been referred to as progesterone intolerance which can present as mood changes, irritability, fatigue or feelings of depression after starting progesterone therapy. The mechanisms behind this are not fully understood but may relate to individual differences in how progesterone is metabolised into neuroactive compounds in the brain.
For some women simply changing the formulation or route of administration can make a significant difference. Options may include lowering the dose, using vaginal progesterone instead of oral, changing the timing of the dose or trying a different progesterone regimen.
Because progesterone is essential for protecting the uterine lining in women taking oestrogen, it is important that any intolerance is managed rather than simply discontinuing treatment.
Our Advanced Hormone Test is unique in the fact that it doesn’t just look at progesterone levels, it also assess which metabolites are being made. Progesterone is metabolised down two pathways, resulting in two distinct metabolites. Of these, 5a-pregnanediol is the preferred metabolite. This is because it has the ability to cross the blood-brain barrier and enhance GABA activity. Consequently, 5a-pregnanediol is more often linked to progesterone’s beneficial effects than the other metabolite, 5b-pregnanediol. Women who utilise this more favourable metabolic pathway may also experience better tolerance for exogenous progesterone.
6. Ignoring diet and lifestyle changes
Hormones do not operate in isolation. Lifestyle factors such as sleep, nutrition and stress levels can have a significant influence on how women experience perimenopause and how well HRT works. Poor sleep, high alcohol intake, excess caffeine and unstable blood sugar levels can all worsen symptoms such as anxiety, hot flushes and fatigue.
Research also shows that the hypothalamic pituitary adrenal (HPA) axis, the system that regulates our stress response, becomes more sensitive during the menopausal transition. Elevated cortisol levels associated with chronic stress can produce symptoms that overlap with perimenopause including fatigue, low mood, poor sleep, reduced libido and anxiety. If these underlying lifestyle factors are not addressed, HRT alone may not fully resolve symptoms.
Simple foundational strategies can make a meaningful difference. These may include improving sleep hygiene, reducing alcohol intake, supporting balanced meals that stabilise blood sugar and incorporating stress reduction practices such as exercise, mindfulness or relaxation techniques.
HRT often works best when it is part of a broader approach to health rather than a standalone solution. Our Advanced Hormone Test comes with a 3 month personalised health plan which includes diet, lifestyle and supplement recommendations from an expert nutritional therapist to help give you the strong foundations to support HRT treatment.
7. Keeping your dose static throughout perimenopause
Finally, it is important to remember that hormone therapy is not static. Perimenopause is a dynamic process in which hormone levels fluctuate over several years before settling into postmenopause. As a result the dose and type of HRT that works well at one stage may not remain appropriate later. At our bHRT clinic, we recommend regular review of HRT around every 6 months or sooner if symptoms change.
Monitoring allows clinicians to assess symptom response, side effects, bleeding patterns and changes in health status. Adjustments may involve altering the oestrogen dose, changing the progesterone regimen or switching to a different delivery method. It may also include adding in or using different hormones to help alleviate symptoms, such as DHEA or testosterone, for a fully personalised HRT regimen
Regular follow up ensures that HRT remains both safe and effective as a woman moves through different stages of the menopausal transition.
A more personalised approach to HRT
HRT has helped millions of women navigate the challenges of menopause and when used appropriately it remains one of the most effective treatments available. However hormones interact with many systems in the body and the same treatment will not work in exactly the same way for everyone.
Understanding the potential pitfalls of HRT allows women to approach therapy with realistic expectations and encourages a more personalised approach. Factors such as progesterone choice, hormone dosing, metabolism, gut health, lifestyle and ongoing monitoring all play a role in determining how well treatment works.
At FUTURE WOMAN, our specialist bHRT clinic combines in-depth hormone testing with expert prescribing to create a treatment plan that actually works for you.
References
Cavalieri, E. L., & Rogan, E. G. (2010). Depurinating estrogen-DNA adducts in the etiology and prevention of breast and other human cancers. Future Oncology, 6(1), 75–91. https://doi.org/10.2217/fon.09.137
Džidić-Krivić, A., Kusturica, J., Sher, E., Selak, N., Osmančević, N., Farhat, E., & Sher, F. (2023). Effects of intestinal flora on pharmacokinetics and pharmacodynamics of drugs. Drug Metabolism Reviews, 55, 126 – 139. https://doi.org/10.1080/03602532.2023.2186313.
Fuhrman, B. J., Schairer, C., Gail, M. H., Boyd-Morin, J., Xu, X., Sue, L. Y., Buys, S. S., Isaacs, C., Keefer, L. K., Veenstra, T. D., Berg, C. D., Hoover, R. N., & Ziegler, R. G. (2012). Estrogen metabolism and risk of breast cancer in postmenopausal women. Journal of the National Cancer Institute, 104(4), 326–339. https://doi.org/10.1093/jnci/djr531
Gompel, A., & Plu-Bureau, G. (2018). Progesterone, progestins and the breast in menopause hormone therapy. Climacteric, 21(4), 326–332. https://doi.org/10.1080/13697137.2018.1476483
Kwa, M., Plottel, C. S., & Blaser, M. J. (2016). The intestinal microbiome and estrogen receptor-positive female breast cancer. Journal of the National Cancer Institute, 108(8). https://doi.org/10.1093/jnci/djw029
National Institute for Health and Care Excellence. (2015). Menopause: Diagnosis and management (NG23). https://www.nice.org.uk/guidance/ng23
Panay, N., Hamoda, H., Arya, R., & Savvas, M. (2020). The 2020 British Menopause Society recommendations on hormone replacement therapy. Post Reproductive Health, 26(4), 181–209.
Plottel, C. S., & Blaser, M. J. (2011). Microbiome and malignancy. Cell Host & Microbe, 10(4), 324–335. https://doi.org/10.1016/j.chom.2011.10.003
Prior, J. C. (2018). Progesterone for symptomatic perimenopause treatment. Gynecological Endocrinology, 34(6), 443–446. https://doi.org/10.1080/09513590.2018.1441867
Reddy, D. S. (2010). Neurosteroids: Endogenous role in the human brain and therapeutic potentials. Progress in Brain Research, 186, 113–137. https://doi.org/10.1016/B978-0-444-53630-3.00008-7
Santoro, N., Roeca, C., Peters, B. A., & Neal-Perry, G. (2021). The menopause transition: Signs, symptoms, and management options. The Journal of Clinical Endocrinology & Metabolism, 106(1), 1–15. https://doi.org/10.1210/clinem/dgaa764
Santoro, N., & Randolph, J. F. (2011). Reproductive hormones and the menopause transition. Obstetrics and Gynecology Clinics of North America, 38(3), 455–466. https://doi.org/10.1016/j.ogc.2011.05.004
Vinarov, Z., Abdallah, M., Agúndez, J., Allegaert, K., Basit, A., Braeckmans, M., Ceulemans, J., Corsetti, M., Griffin, B., Grimm, M., Keszthelyi, D., Koziolek, M., Madla, C., Matthys, C., McCoubrey, L., Mitra, A., Reppas, C., Stappaerts, J., Steenackers, N., Trevaskis, N., Vanuytsel, T., Vertzoni, M., Weitschies, W., Wilson, C., & Augustijns, P. (2021). Impact of gastrointestinal tract variability on oral drug absorption and pharmacokinetics: an UNGAP review.. European journal of pharmaceutical sciences : official journal of the European Federation for Pharmaceutical Sciences, 105812 . https://doi.org/10.1016/j.ejps.2021.105812.
Zahid, M., Gaikwad, N. W., Rogan, E. G., & Cavalieri, E. L. (2007). Inhibition of depurinating estrogen-DNA adduct formation by natural compounds. Chemical Research in Toxicology, 20(12), 1947–1953. https://doi.org/10.1021/tx700269s
Zhang, X., Han, Y., Huang, W., Jin, M., & Gao, Z. (2020). The influence of the gut microbiota on the bioavailability of oral drugs. Acta Pharmaceutica Sinica. B, 11, 1789 – 1812. https://doi.org/10.1016/j.apsb.2020.09.013.



